Das Patientenvolumen der Mauerseglerklinik (bzw. früher: "Mauerseglerstation") stieg in den Anfangsjahren stetig an und pendelte sich von 2003 bis 2009 zwischen 500 und 700 Seglern pro Saison ein. 2010 wurde die 700er-Marke erstmals überschritten. Seit dieser Zeit ist die Klinik zudem das ganze Jahr über belegt - es gibt kein "Saisonende" und keine "Winterpause" mehr. 2012 sowie 2013 folgte deutlich die 800er-Marke. Seitdem pendeln sich die Zahlen zwischen 700 und 800 Patienten jährlich ein. Dies ist der Tatsache geschuldet, dass viele schwer geschädigte Patienten - vor allem solche mit Gefiederschäden - monatelang aufwändig in der Mauerseglerklinik behandelt werden. Ist die Klinik mit Patienten ausgelastet und „kein Bett frei“ können keine neuen Segler angenommen werden.
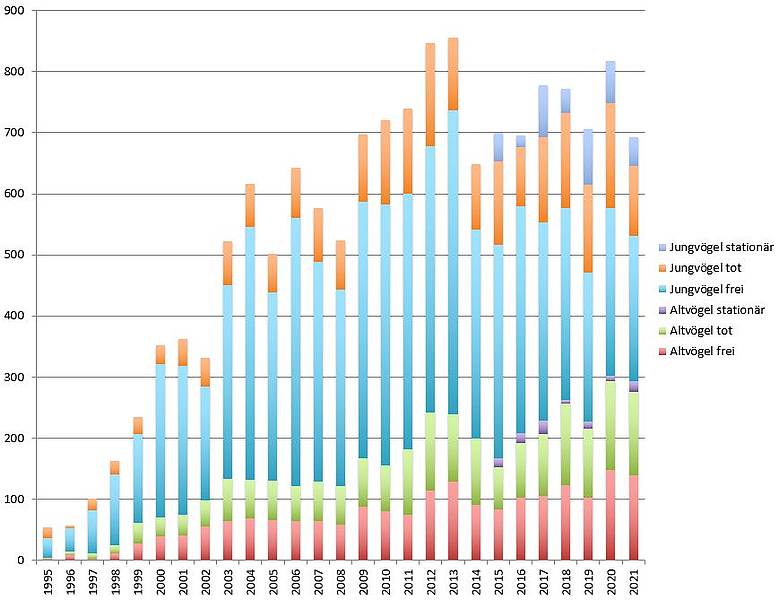
Die Fluktuationen ab 2003 sind einerseits durch Umweltfaktoren begründet, die sich auf das (Brut-)Verhalten der Mauersegler auswirken. In besonders heißen Jahren springen beispielsweise mehr Jungvögel aus ihrem Nest, um dem Hitzetod zu entgehen. Entsprechend werden mehr hilfsbedürftige Jungvögel gefunden und in die Klinik gebracht. Dies gilt gleichermaßen für kalte und nasse Jahre, wobei in diesen Jahren stark abgemagerte Tiere gefunden werden. In beiden Fällen - große Hitze und Dauerregen - geht gleichzeitig das Insektenaufkommen zurück. Adulte wie juvenile Segler magern ab. Seit 2017 gehört zum Allgemeinwissen, dass es aber auch bei guter Wetterlage immer weniger Insekten gibt. Dies ist dem Einsatz von Giften in der Landwirtschaft und den Kleingärten ebenso geschuldet wie einer weitgehend monokulturellen Landwirtschaft, die zudem Feldwege versiegelt und Feldraine nicht duldet. Auch darunter leiden Mauersegler wie auch andere Vögel.
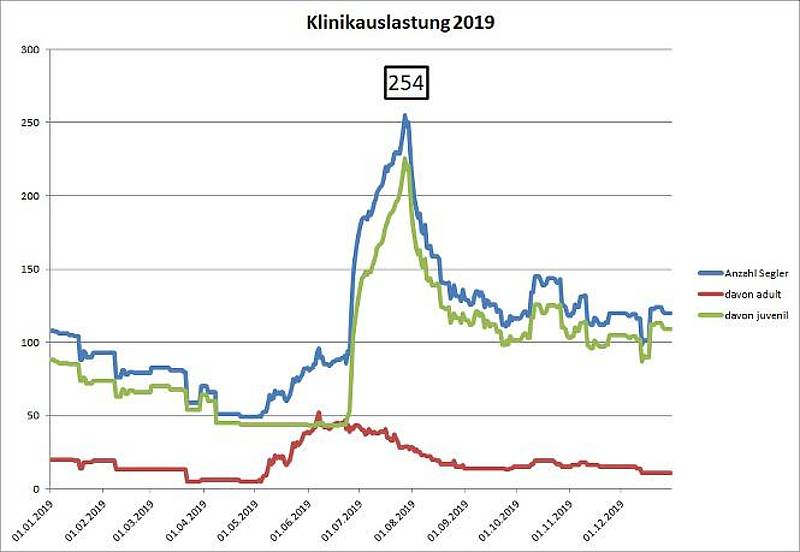
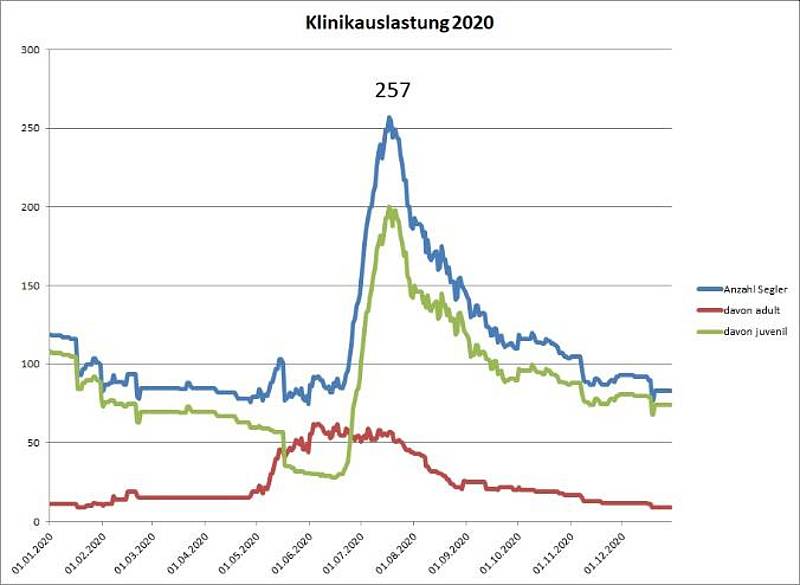
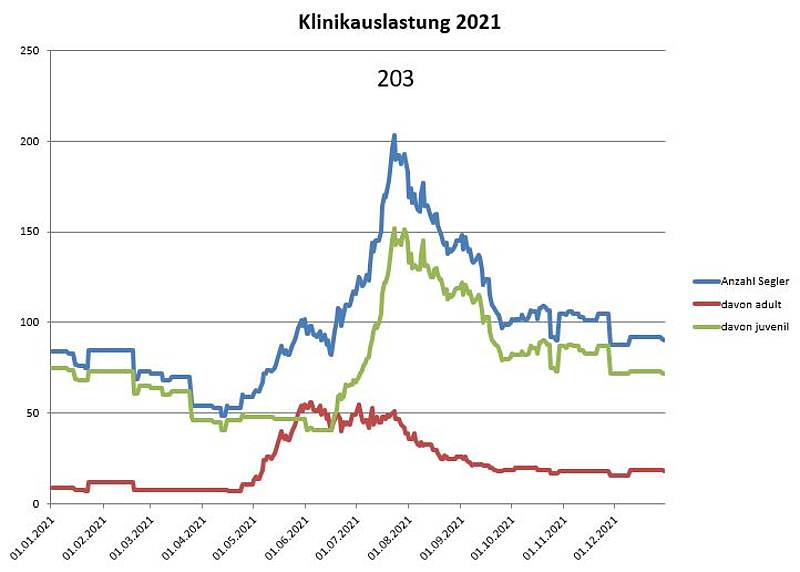
Zudem musste die Klinik seit 2007 temporäre Aufnahmestopps verhängen, weil die Kapazitätsgrenzen schlichtweg gesprengt wurden. Die folgenden Grafiken zeigen die tägliche Auslastung der Mauerseglerklinik in den Jahren 2018 - 2021. Obwohl zur Abfederung von Belastungsspitzen die Aufzucht unverletzter Nestlinge teilweise in kompetente, ausgewählte Pflegestellen verlagert wurde, kam es beispielsweise 2012 wieder zu einer Spitzenauslastung von über 250 Seglern. In den Zahlen des Jahres 2013 spiegelt sich wider, dass der Sommer in 2013 kalt und nass war. Deshalb konnten Mauersegler oft nicht direkt nach dem Flüggewerden starten. Gleichzeitig wurden stetig neue Segler eingeliefert. In 2014 wurden ebenfalls Spitzenwerte von über 240 stationären Patienten erreicht. Trotz der großzügigen Räume erfordern diese Zahlen nach wie vor eher die Selbstaufgabe als ein einfaches Engagement der KlinikmitarbeiterInnen - auch, weil durch die "Umleitung" der unkomplizierten Jungvögel in Pflegestellen die verbleibenden Patienten kompliziertere Fälle darstellen. So werden Altvögel nach Möglichkeit immer aufgenommen, weil ihre Behandlung in der Regel spezielles Wissen und Können erfordert. Junge Mauersegler mit Gefiederschäden, wie sie sich nach dem Flüggewerden der Vögel zeigen können, müssen in den Pflegestellen bleiben, bis die Kapazitäten der Klinik ausreichen, sie aufzunehmen. Gefiedergeschädigte Segler aus privater Hand werden nach Möglichkeit in ausgewählte Pflegestellen vermittelt oder direkt in der Klink aufgenommen.
Die Tabellen zeigen zudem, dass in den letzten Jahren mit immer mehr Patienten schon in eine neue Saison gestartet wird. Dies ist der Tatsache geschuldet, dass die Mauerseglermauser von juvenilen Patienten erst im zweiten Lebensjahr stattfindet und adulte Mauersegler erst im April/Mai mit der Mauser durch sind; es gibt aber auch Mauersegler, die sehr lange auf eine Übernahme warten müssen. Rechtfertigen lässt sich ein so langer Aufenthalt in Menschenhand nur damit, dass Mauersegler grundsätzlich lange leben können und ihre Fähigkeiten, sich in Freiheit behauten zu können, nicht verlieren.

| Jahr | Altvögel frei | Altvögel tot | Altvögel stationär | Jungvögel frei | Jungvögel tot | Jungvögel stationär | Summe |
|---|---|---|---|---|---|---|---|
| 1994 | 0 | 1 | 6 | 7 | 14 | ||
| 1995 | 2 | 2 | 33 | 17 | 54 | ||
| 1996 | 9 | 5 | 38 | 5 | 57 | ||
| 1997 | 3 | 8 | 71 | 19 | 101 | ||
| 1998 | 11 | 13 | 117 | 22 | 163 | ||
| 1999 | 27 | 34 | 146 | 27 | 234 | ||
| 2000 | 39 | 31 | 251 | 31 | 352 | ||
| 2001 | 41 | 33 | 244 | 44 | 362 | ||
| 2002 | 56 | 42 | 187 | 47 | 332 | ||
| 2003 | 64 | 69 | 317 | 72 | 522 | ||
| 2004 | 69 | 63 | 413 | 71 | 616 | ||
| 2005 | 66 | 64 | 308 | 64 | 502 | ||
| 2006 | 65 | 57 | 439 | 81 | 642 | ||
| 2007 | 65 | 64 | 360 | 87 | 576 | ||
| 2008 | 58 | 64 | 321 | 80 | 523 | ||
| 2009 | 88 | 79 | 420 | 110 | 697 | ||
| 2010 | 81 | 75 | 427 | 138 | 721 | ||
| 2011 | 75 | 107 | 418 | 140 | 741 | ||
| 2012 | 114 | 128 | 437 | 168 | 847 | ||
| 2013 | 129 | 110 | 497 | 120 | 3 | 859 | |
| 2014 | 91 | 109 | 10 | 341 | 107 | 34 | 692 |
| 2015 | 83 | 70 | 14 | 350 | 136 | 47 | 700 |
| 2016 | 102 | 90 | 16 | 371 | 97 | 20 | 696 |
| 2017 | 105 | 101 | 23 | 324 | 140 | 85 | 778 |
| 2018 | 123 | 134 | 6 | 314 | 155 | 40 | 772 |
| 2019 | 103 | 113 | 11 | 244 | 143 | 92 | 706 |
| 2020 | 148 | 145 | 9 | 275 | 171 | 69 | 817 |
| 2021 | 139 | 136 | 18 | 238 | 114 | 47 | 692 |
Die eingelieferten Vögel kommen aus ganz Deutschland und dem europäischen Ausland, mit einem Schwerpunkt im Rhein-Main-Gebiet. 2021 zum Beispiel kamen Mauersegler, Alpen- und Fahlsegler aus Polen, Österreich, Rumänien, Belgien, Italien, Frankreich, Spanien und der Schweiz.
Knapp ein Drittel aller Patienten wird von anderen Institutionen überwiesen, darunter hauptsächlich Pflegestellen, Tierheime und Tierärzte/-kliniken. In den meisten Fällen wandten sich die Finder jedoch direkt an die Mauerseglerklinik.
Die Aufenthaltsdauer unserer Mauersegler-Patienten betrug 2021 bei erfolgreich freigelassenen im arithmetischen Mittel 31,4 Tage, im Median 23 Tage. Die starken Differenzen zwischen arithmetischem Mittel und Median werden durch die Langzeitpatienten verursacht, die das arithmetische Mittel nach oben verzerren. Die untenstehende Abbildung zeigt die Gesamtwerte aller Mauersegler. Eine tiefer gehende Unterscheidung nach Adulten und Juvenilen enthüllt, dass die meisten freigelassenen adulten Mauersegler bereits nach kurzer Zeit (14 Tage) die Klinik verlassen konnten, während juvenile Segler im Mittel 26 Tage bis zur Freilassung versorgt wurden. Diese Zahlen spiegeln natürlich die Aufzucht wieder. Auffällig ist auch, dass die Entscheidung zur Euthanasie für adulte Segler im Median bereits nach 2 Tagen Klinikaufenthalt fällt, während es bei juvenilen Seglern 14 Tage sind. Grund hierfür ist, dass adulte Segler häufig mit schwersten Verletzungen eingeliefert werden und daher vielfach keine Chance zur Rettung besteht. Bei juvenilen Seglern sind die Gründe hingegen anders gelagert, z.B. durch zeitverzögert auftretende Folgeschäden von Fehlernährung beim Finder. Verletzungen spielen hier eine geringere Rolle, doch zeigt sich auch bei einzelnen juvenilen Patienten bei den ersten Flugversuchen im Trainingsraum, dass sie bei ihrem Sturz aus dem Nest Verletzungen erlitten haben, die nun erst erkannt werden können. Die Hohe Diskrepanz zwischen arithmetischem Mittel und Median verdeutlicht jedoch, dass die Entscheidung zur Euthanasie in jedem Einzelfall gründlich überdacht und reiflich überlegt getroffen wird. Einzelne Patienten mit unsicherer Prognose werden über längere Zeiträume beobachtet und therapiert, was das arithmetische Mittel nach oben verzerrt.