Als Notfallpatient gilt jeder Mauersegler, dessen Zustand keinen vollständigen klinischen Untersuchungsgang, sondern vorerst nur eine fraktionierte Untersuchung gestattet, und der als instabil bis unmittelbar lebensbedrohlich eingestuft wird. Vor Vervollständigung des Untersuchungsganges sind lebenserhaltende Sofortmaßnahmen erforderlich.
Dazu zählen:
- Unfallvögel mit Schock und/oder schwerem Trauma,
- Mauersegler mit profusen Blutungen,
- Hochgradig abgemagerte und/oder exsikkotische adulte Segler,
- Hochgradig abgemagerte und / oder exsikkotische Nestlinge,
- Mauersegler mit hochgradiger Dyspnoe,
- Längerfristig und schwerst fehlernährte Segler mit hochgradigen Allgemeinstörungen,
- Mauersegler mit hochgradigen Allgemeinstörungen unbekannter Genese,
- Mauersegler mit Defekten des Groß- und/oder Körpergefieders, die unmittelbare und möglicherweise lebensbedrohliche Auswirkungen auf das Allgemeinbefinden haben.
Erste-Hilfe-Maßnahmen bei Notfallpatienten
Dyspnoe:
- Den Rachen kontrollieren, etwaige mechanische Atemhindernisse entfernen (z.B. Blut, Speichel, Schleim, hochgewürgtes Futter).
- Bei rasselnden, schmatzenden Atemgeräuschen: Furosemid in einer Dosierung von 1 bis max. 2 mg/kg KM p.o. oder i.m.; bei Wiederauftreten kann die Applikation an den nachfolgenden zwei bis drei Tagen wiederholt werden. Die Gefahr einer anschließenden Exsikkose ist zu beachten.
- Bei aussetzender Atmung tropfenweise perorale Verabreichung von Dimethylbutyramid als peripheres Atemstimulans. Tropfen nie direkt in den Schlund applizieren (Gefahr einer Aspirationspneumonie), sondern auf der ventralen Rachenschleimhaut verstreichen.
- Bei Atemstillstand Reanimationsversuche mit Doxapram tropfenweise per os oder in einer Dosierung von 10 mg/kg KM intramuskulär.
- Bei hochgradiger Dyspnoe (würgende, fiepsende Atemgeräusche, Erstickungsanfälle) ohne Ansprechen auf die genannten Atemstimulantien sollte der Vogel ohne weiteres Zuwarten eingeschläfert werden.
Schock:
Zur Volumensubstitution im Schock bewährt sich die subkutane Verabreichung (Kniefalte) von 0,8 - 1 ml körperwarmer Ringer-Lactat-Lösung pro Vogel. Ferner erhalten Schockpatienten einmalig Kortikosteroide intramuskulär (Prednisolon 5 mg/kg KM).
Kachexie / Exsikkose:
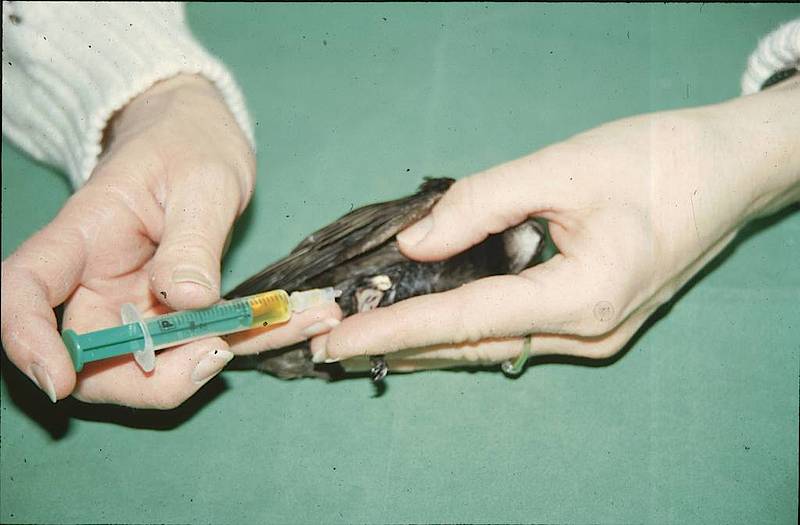
Zur Volumensubstitution und Kreislaufstabilisierung wird 0,8 - 1 ml Amynin / Ringer-Lactat im Verhältnis 1:1 körperwarm subkutan appliziert, gegebenenfalls zwei- bis dreimal im Abstand von jeweils acht bis zwölf Stunden. Handelsüblicher, warmer Kaffee, ungefähr 15-20 Minuten nach der Infusion tropfenweise eingeflößt, erweist sich vielfach als ein schonendes und wirkungsvolles Kreislaufstimulans.Bei Kreislaufversagen ist Etilefrinhydrochlorid (0,2 - 1 mg/kg KM i.m. oder p.o.) und g-Strophantin (tropfenweise p.o.) angezeigt. Bei metabolischer Azidose nach langen Hungerphasen empfiehlt sich die einmalige subkutane Gabe von Natriumbicarbonat 4,2 % in einer Dosierung von 15 ml / kg KM.
Hypothermie:
í„ußerliche Wärmezufuhr (30 - 35° C) durch Heizdecke, Rotlicht oder einen Infrarot-Dunkelstrahler ist für den Intensivpatienten unerlässlich. Fütterungs- oder Tränkversuche von Notfallpatienten sind bis zur Stabilisierung von Atmung und Kreislauf nicht indiziert. Die Versorgung mit Flüssigkeit und Nährstoffen kann mittels subkutan verabreichter Roborantien über einen Zeitraum von 12 - 24 Stunden parenteral erfolgen.
Krämpfe und Konvulsionen:
Die intramuskuläre Verabreichung von Diazepam in einer Dosierung von 5 mg/kg KM kann hilfreich sein. Ferner empfiehlt sich bei Schädeltrauma (Commotio cerebri) und zentralnervösen Störungen die einmalige Gabe von Vitamin-B-Komplex (10 - 30 mg/kg KM i.m. oder s.c.; der Gehalt von Vit. B1 darf 5 mg/kg KM nicht überschreiten).
Blutungen:
Das Stillen von Blutungen erfolgt je nach Lokalisation durch Fingerdruck, Druckverband, lokale (Eisen-III-Chlorid oder Silbernitrat-Stift topisch) und/oder systemische Hämostyptika (Naphthionsäure 100 mg/kg KM i.m.).
Offene Wunden / Frakturen:
Sofern keine infauste Prognose: Wundtoilette / Ostesynthese unter Allgemeinanästhesie. Es gelten dieselben Voraussetzungen und Anforderungen an eine chirurgische Wund-/Frakturversorgung wie in der Kleintiermedizin!!
Ist der Patient nicht narkosefähig, kann die Wundversorgung nicht gleich vorgenommen werden: sterile Wundabdeckung / vorläufige Fixation. Austrocknen von Gewebe und Knochen unbedingt vermeiden. Analgetika verabreichen!
Augenverletzungen:
Analgetika systemisch und lokal. Mit einer ophthalmologischen Untersuchung beim Spezialisten schnellstmöglich abklären, ob die Sehfähigkeit des Auges wiederherzustellen ist. Ansonsten umgehend Euthanasie.
Gefiederverschmutzung:
Bei hochgradiger Gefiederverschmutzung kann versucht werden, unter Allgemeinanästhesie zunächst mit körperwarmem Wasser und handelsüblichen Spülmitteln eine vorläufige Reinigung zu erzielen und eine mögliche perorale Fremdstoffaufnahme durch den Vogel, etwa bei Putzversuchen, zu unterbinden. Möglichst frühzeitig muss eruiert werden, mit welcher verschmutzenden Substanz man es zu tun hat, um ein geeignetes Detergenz zur Reinigung zu finden. Vorsicht: Viele Reinigungs- und Lösungsmittel sind hochgradig toxisch für den Patienten!